
Learn the Ankle replacement-Revision using Wright Invision Ankle replacement system surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the Ankle replacement-Revision using Wright Invision Ankle replacement system surgical procedure.
With increasing numbers of total ankle arthroplasty (TAA) operations being carried out worldwide it can be expected that we are going to encounter more frequent and probably more complex failure situations. Failure of ankle replacements occurs due to a variety of causes and some risks for early failure have been established in the literature, Gadd et al. Over time it can be considered that wear will generate a cytokine response and bone lysis, leading to implant migration and cyst formation. This mode of failure is more frequently seen in certain makes of TAA with the best know example being the now withdrawn AES system which generated massive osteolysis in some series .
The origin of cysts and loosening has been widely debated. Rodriguez et al. (2010) hypothesized that cyst formation may be related to pump action leading to synovial inclusion. However Bonnin et al. (2011) felt that some of the cysts may have evolved from pre-existing arthritic cysts. Jacobs et al. (2006) hypothesized that cyst formation may be related to overwhelming of a local afferent transport mechanism with wear particles, resulting in an accumulation of wear particles in periprosthetic tissue. Finally repeatedly authors have failed to find significant wear particles in retrieval specimens from the cysts but some (Koivu et al) have found that there is a switching on of an inflammatory cascade concluding that there is an increased expression of ‘high-mobility group box 1’ receptor for advanced glycation end product and other ‘danger signals’ which could contribute to inflammation around the implants, multilocular cyst formation, and osteolysis in failed TAA implants
The Mobility TAA (DePuy) was launched in 2003 and was withdrawn in June 2014 . There have been no widespread publications of osteolysis though persistent medial pain is reported in some patients.
For failed TAA the commonest option is to convert the arthroplasty to an arthrodesis, which is an accepted and successful technique. Bone graft is often used from the fibula, iliac crest, allograft or using bone substitutes to fill the resulting bone void from where the implant has been removed. If union occurs then pain relief will usually follow, but so does stiffness. If the bone loss is significant then the subtalar joint will often also be sacrificed with even greater loss of motion and functional deficit. Preservation of the subtalar joint is technically possible, usually requiring grafting of the talar defect and plate fixation of the ankle joint, if enough talar bone stock remains.
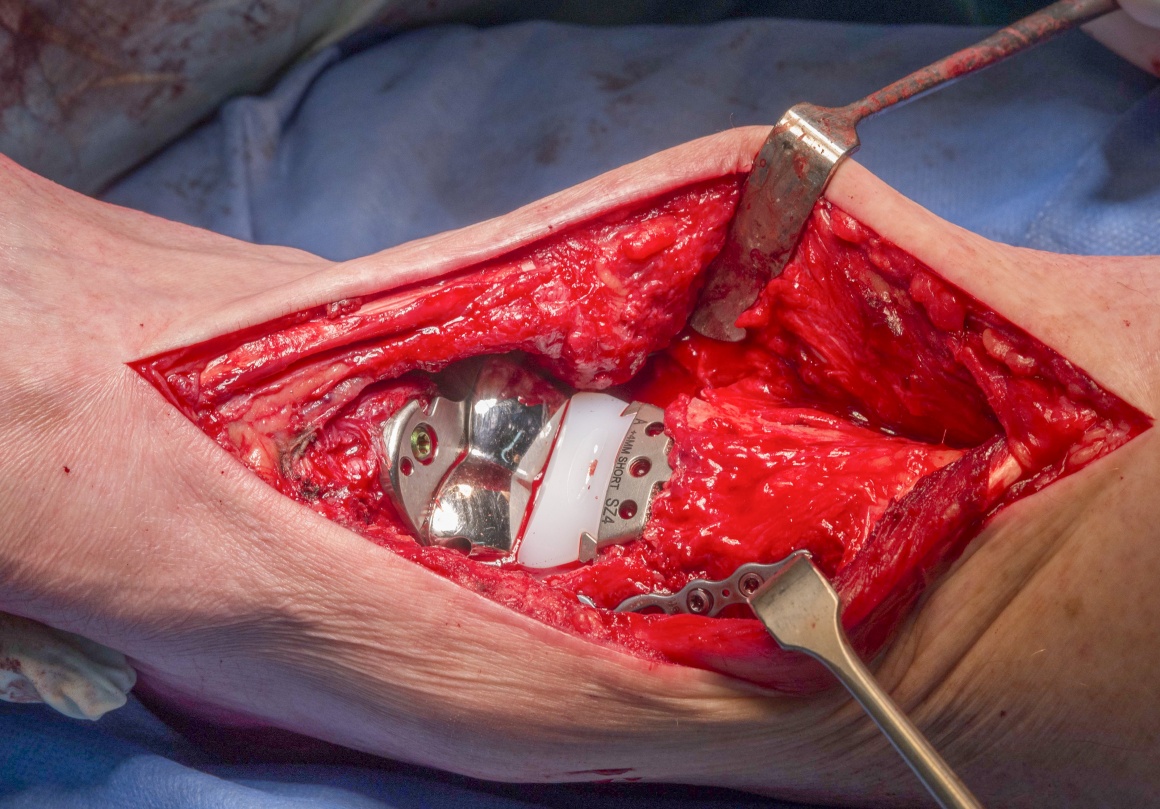
The alternative, in order to preserve motion, is to convert the failed arthroplasty to a revision joint replacement. Specific equipment has now come on to the market to facilitate this. The most tried and tested of these is the InBone system from Wright Medical Technologies, USA. There are publications that support its efficacy at early follow up (Devries, et al). The InBone is a fixed point, jig driven system using image intensification throughout in order to position the revision replacement in a reliable orientation. The system has been added to in the InVision System which also gives metallic solutions to bone loss by use of bulkier tibial trays and talar domes and with the addition of a flat plate to the talus, allowing bridging of cyst defects in the talus. The plate has augments which can be added to the plantar talar surface, though they are limited by their position.
Detailed is a complex revision of a Mobile bearing De Puy Mobility Total Ankle Arthroplasty (which failed due to cyst formation) revised to a fixed bearing InVision Ankle replacement. The case is complicated by bony deficiency of the talus and fracture of the medial malleolus both of which are treated and discussed.
Gadd RJ, Barwick TW, Paling E, Davies MB, Blundell CM. Assessment of a three-grade classification of complications in total ankle replacement. Foot Ankle Int. 2014;35(5):434-437.
Kokkonen A, Ikavalko M, Tiihonen R, et al. High rate of osteolytic lesions in medium-term followup after the AES total ankle replacement. Foot Ankle Int. 2011 Feb;32(2):168-75.
Author : Mr Chris Blundell FRCS (Tr & Orth)
Institution :The Northern general hospital ,Sheffield ,UK.
Clinicians should seek clarification on whether any implant demonstrated is licensed for use in their own country.
In the USA contact: fda.gov
In the UK contact: gov.uk
In the EU contact: ema.europa.e

INDICATIONS
Ankle replacements which initally provide good range of motion and pain relief may later start to fail. This is indicated by increasing pain and/or the presence of loosening or cysts on plain radiographs. This asymptomatic loosing or cyst formation is of concern to those conducting TAA as part of their practice. I would encourage the long term regular review of patients clinically and with radiographs to spot problems early.
SYMPTOMS & EXAMINATION
Patients may demonstrate swelling which is new and pain which may initially be intermittent but gradually becomes more persistent. The pain may be poorly localised. It is important to take a full history especially focussing on any history of poor wound healing after the index procedure which might raise concern about the possibility of low grade sepsis. Blood tests to help exclude this will include a white cell count (WCC) , C reactive protein (CRP) assay and eosinophil sedimentation rate (ESR). Elevation of any of these will raise further concern which will lead to a biopsy to look for infecting organisms. If present then a revision to fusion as a two stage procedure is recommended rather than to a further TAA which is contraindicated.
IMAGING
Plain radiographs as AP and lateral images are the mainstay and are used to provide image surveillance of TAA. Plain radiographs should be examined for implant migration, loosening and cysts. Certain models of ankle replacement have a high incidence of mobile bearing failure, such as the STAR system, and for this reason metal markers are put in the radiolucent polyethylene bearings, these should remain orthogonal and not show any motion year on year.
If the patient has symptoms as described above then a CT scan should be done. This will characterise any areas of poor integration and the all important presence of cysts which may be very difficult see on plain imaging. If sepsis is suspected then SPECT CT has gained popularity but beware that theses images will show increased activity for at least a year post index operation due to healing occurring at the implant bone interface.
ALTERNATIVE OPERATIVE TREATMENT
Cysts may be treated by curettage and grafting with autologous bone or bone substitutes. There are publications supporting this treatment but in the authors experience these cysts tend to reoccur. Gross et al from Duke University examined a series of grafted cysts with 90% good result at 24 months but this fell to 60% at 4 years. If the cysts are in such a position that the structural support of the implant is at risk then even if asymptomatic I will suggest to the patient that these cysts should undergo debridement. I have treated them with installation of bone cement particularly in the lower demand individual.
NON-OPERATIVE MANAGEMENT
Observation of the cysts may be reasonable to see if there is progress in terms of size. Once seen, the cysts do cause concern and radiographic surveillance is mandatory. I do this with the use of CT scans as the assessment is more accurate. Progressive cysts lead me to consider intervention using shared decision making with the patient who may be asymptomatic and so this conversation can be a difficult one.
CONTRAINDICATIONS
The presence of sepsis as discussed above is a complete contraindication to revision TAA. If after CT the cysts are just too extensive or bone loss too great then I would advocate a revision to a fusion with appropriate use of bone graft.
This 68 year old male who is a keen golfer, had had a successful Mobility mobile bearing total ankle replacement 10 years ago for primary ankle osteoarthritis. A cyst had been noted for the previous 18 months without symptoms. In the last 3 months there has been increasingly severe pain and loss of mobility. Plain radiographs show the cyst and its progressive nature. CT scans were performed to gather further information regarding the cyst. The increasing pain is suspicious for the talus neck having become incompetent mechanically or being frankly fractured.
A full discussion with the patient including the risks of continuing to watch and wait or to intervene. Intervention could take the form of packing the cyst or revision to a fusion or a further TAR. The later option was deemed preferable by both patient and surgeon as discussed above.

The patient is positioned supine. Analgesia was in the form of a general anaesthetic with an epidural for pain relief – the duration of the procedure was difficult to define and so a spinal / epidural was not felt to be ideal.
No antibiotics were given on induction until specimens of the cyst had been taken. Although infection was deemed to be very unlikely I did not want to obscure the value for specimens of both the cyst and the implant interfaces that were subsequently acquired.
A thigh tourniquet is used but not inflated at the outset to conserve tourniquet time for a potentially protracted operation
Draping must expose the knee to ensure rotational alignment is respected. The old wound is marked and can be used for the revision TAR.


























































The patient is rested with the limb elevated for two weeks. I use a factor 10a inhibitor (Rivaroxaban) for thromboprophylaxis as per our risk assessment. The patient takes this every day for 6 weeks for revisions such as this where the surgical time is greater than 90 minutes.
The plaster backslab and sutures are removed at 2 weeks and the patient then starts physiotherapy active and passive range of motion rehabilitation. Full weight bearing mobilisation is permitted in a removable walker boot.
The boot is used until the patient is 6 weeks post op and at that stage a further review with an Xray is carried out. After this full and free mobilisation though often a compression sock is used to help reduce swelling. In this case radiographs at 6 weeks show the medial malleolar fracture to have lots of bridging callus.
Physiotherapy continues for 3 to 6 months.

Gadd RJ, Barwick TW, Paling E, Davies MB, Blundell CM.
Assessment of a three-grade classification of complications in total ankle replacement.
Foot Ankle Int. 2014;35(5):434-437
The authors review a 15 year experience of TAA in one centre, reviewing a 17% failure rate at 15 years in 217 replacements over this period. They retrospectively look at complications and their association with failure. Complications are characterised as high grade >50% risk (deep sepsis, aseptic loosening, implant failure) or low grade <50% risk (Malleolar fractures, wound healing problems, technical malposition) for failure leading to revision to further TAA or arthrodesis.
Kokkonen A, Ikavalko M, Tiihonen R, et al.
High rate of osteolytic lesions in medium-term followup after the AES total ankle replacement.
Foot Ankle Int. 2011 Feb;32(2):168-75.
A two year review demonstrated 79% survival of 38 implants but with 50% showing osteolysis and 24% having large cysts and massive osteolysis at this early stage. The implant was abandoned by the authors because of these concerns.
Koivu H, Takakubo Y, Mackiewicz Z, Al-Samadi A, Soininen A, Peled N, Kukis M, Trokovic N, Konttinen YT.
Autoinflammation around AES Total Ankle Replacement Implants.
Foot Ankle Int. 2015 Dec;36(12):1455-62
A complex paper to read but interesting pathology science around retrieval specimens from cysts in AES implants. The authors go on to characterise certain receptors in these specimens and postulate a mechanism for cyst formation due to an inflammatory mechanism.
Gross CE, Huh J, Green C, Shah S, DeOrio JK, Easley M, Nunley JA.
Outcomes of Bone Grafting of Bone Cysts After Total Ankle Arthroplasty.
Foot Ankle Int 2016 Feb; 37(2):157-164
The authors located cysts in 31 cases on review of more than 700 TAR. Cysts were treated in a variety of methods including autograft, allograft, synthetic material, PRP and cement. Patients images were reviewed at 24 and 48 months. The authors draw no specific advice as to which technique is best for treatment nor have they given specifics as to why the variety of techniques was employed. They have reported cyst fill rates of 90% at 2 years review falling to 60% at 48 months. 2 cases had more tan one surgeries for the same cysts. 4 cases had failed before 2 years with these cases requiring component revision or in one case TTC fusion.
A complex paper to read but interesting pathology science around retrieval specimens from cysts in AES implants. The authors go on to characterise certain receptors in these specimens and postulate a mechanism for cyst formation due to an inflammatory mechanism.
Gross CE, Huh J, Green C, Shah S, DeOrio JK, Easley M, Nunley JA.
Outcomes of Bone Grafting of Bone Cysts After Total Ankle Arthroplasty.
Foot Ankle Int 2016 Feb; 37(2):157-164
Reference
- orthoracle.com



