

Learn the SuperPath® total hip replacement surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the SuperPath® total hip replacement surgical procedure.
The SuperPath® approach for total hip replacement is a muscle sparing approach based on 2 previous techniques, PATH® and SuperCap®. The name SuperPath® is an abbreviation of the anatomical basis of the approach: SupraCapsular Percutaneous Assisted Total Hip. Although it is classed in the family of Superior approaches to the hip, on closer inspection, the approach is the top end of a standard ‘Posterior’ approach using the interval between Piriformis at the back and Gluteus Minimus at the front. Its main benefits are of complete muscle and tendon sparing in its purest form, whilst having the extensibility of the posterior approach at any point during the procedure. This allows both a safe learning curve and a wider range of indications compared to other ‘Muscle sparing approaches’.
It has been proven that patients have less post operative pain and a shorter length of stay with the technique. (reference 1 and 2) Early functional goals are reached faster including, time to coming off crutches, return to driving and return to work. (reference 3)
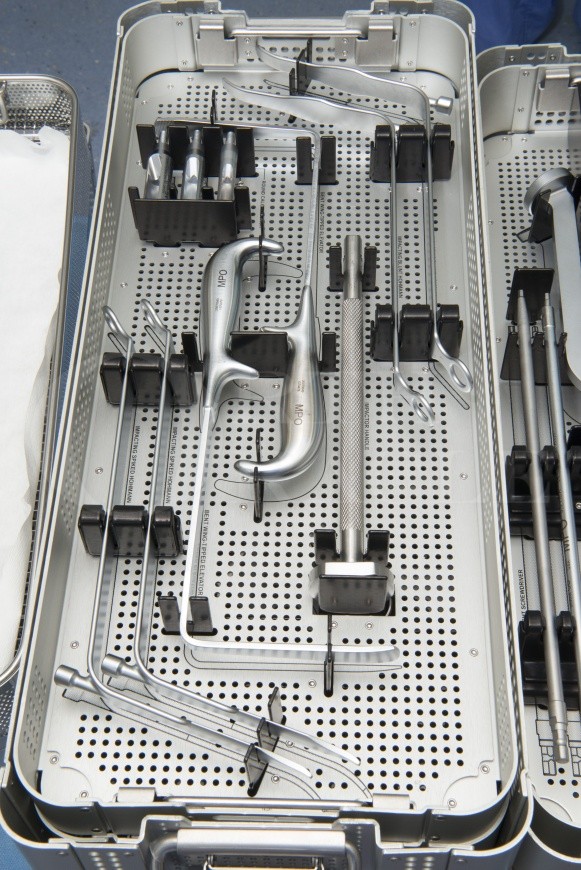
The technique is based around a set of modified instruments that allow direct access to the femur from above and direct access to the acetabulum through a specially designed portal. The use of the portal allows more soft tissue preservation than other superior approaches that rely on offset reamers to access the socket. The instruments come in 2 simple trays that are easy for nursing staff to follow and no additional table attachments are required.

INDICATIONS
The indications are that of any standard Total Hip Replacement. Obviously conservative measures should be exhausted and every case discussed with the patient regarding the balance between benefits of pain relief and improved function, balanced against the risks of surgery.
At present the technique is most suited to the use of uncemented implants. Although technically the approach could be adopted for cemented implants, the surgical instruments are not currently available to assist this. Uncemented implants are available in several philosophies: Short stem, Blade stem, Fully coated tapered stem and canal filling stem. All are available in both modular neck and monolithic stems.
The common difficulties encountered with other tissue sparing or minimally invasive approaches regarding obesity and muscular patients are not as relevant to this technique due to the ability to easily extend.
SYMPTOMS & EXAMINATION
These are the same as for any hip replacement patient with groin pain, anterior thigh pain and buttock pain being the most common. These can initially be treated conservatively but common symptoms for patients at a stage requiring hip replacement include:
Night pain, increased analgesia requirements, reduced walking distance and reduced range of movement. This is often seen with difficulty getting down to feet to put on shoes, difficulty getting in and out of a car and ascending stairs.
Examination findings are of stiffness (including fixed flexion deformity, reduced flexion and particularly internal rotation), joint irritability and muscle weakness (seen on Trendelenburg testing or manifest as a limp). Leg length discrepancy is important to note so it can be accurately corrected during surgery.
IMAGING
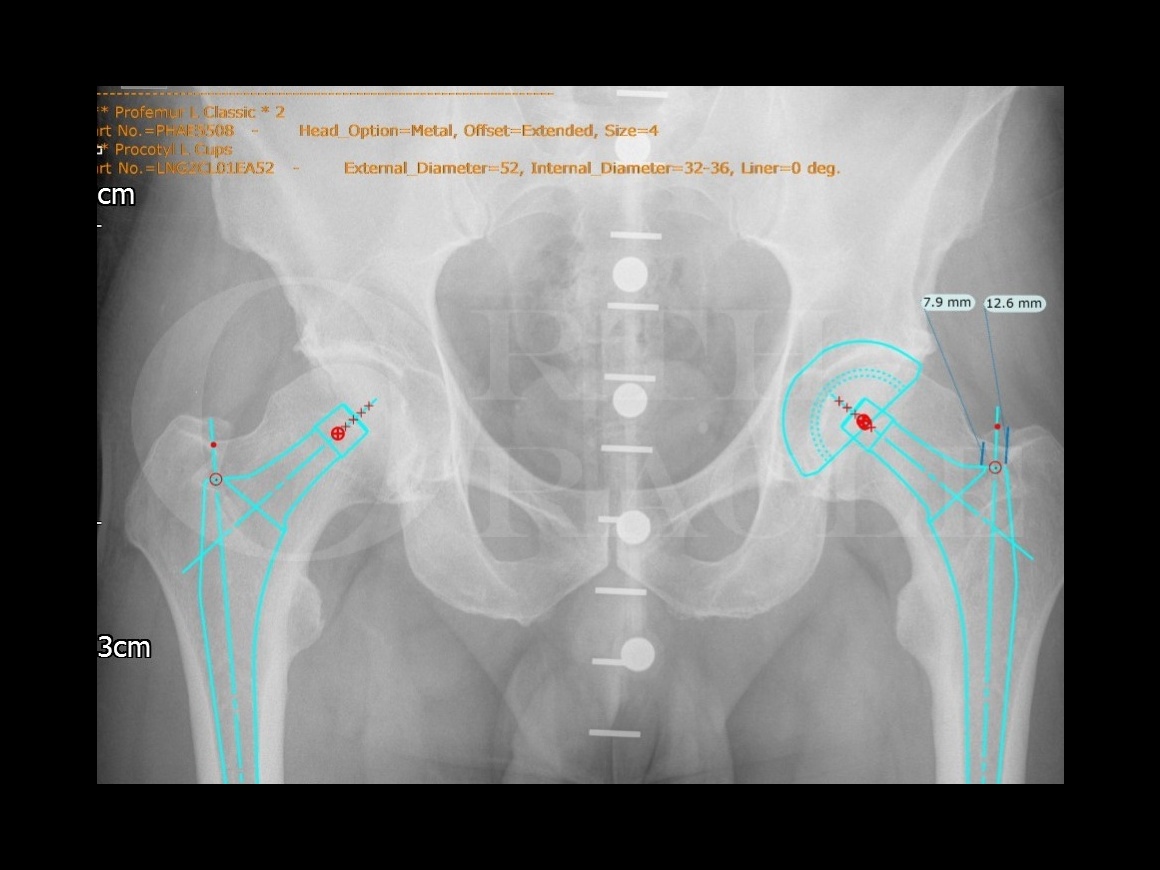
A pre-operative x-ray with scaling marker is essential to make a pre-operative plan. Once the implants are positioned in a standard fashion (to reproduce length and offset) the distance of the femoral stem from the tip of the greater trochanter is measured.
ALTERNATIVE OPERATIVE TREATMENT
This approach can be easily extended by releasing the short external rotators and posterior capsule in a sequential fashion until the approach is the same as a full posterior approach
CONTRAINDICATIONS
The contraindications for the approach are the same as the absolute contraindications for any total hip replacement (presence of infection, bone tumours, severe muscle of nerve dysfunction of the lower limb, bone stock deficiency or severe medical comorbidity)
Relative contraindications depend on the level of surgeon experience but, as the approach can easily be extended by releasing the posterior structures sequentially until you have a full posterior approach, it is possible to start any case requiring THR using this approach. Although initially obesity and very muscular patients are more difficult to treat, as experience is gained, I personally feel that the approach is as easy if not easier than a standard posterior approach.
Author: Mr Michael Cronin BSc, MBBS, FRCS (Tr & Orth)
Institution : Morriston Hospital, Swansea, UK.

The patient is set up as for any Total Hip Replacement. Local policies should be followed for DVT prophylaxis, Antibiotics and Tranexamic acid.
Anaesthetic is again down to surgeon/anaesthetist preference. Initially you should be aware that it may take additional time to perform the procedure but again the approach can always be extended if necessary to negate this. It has been proven that surgical time improves quickly during the learning curve. ( reference 4)
The patient is positioned in a standard lateral decubitus position using the surgeons preference of hip supports (my preference is a double support on both ASIS and a single posterior support on the sacrum). Care must be taken to allow a full range of movement including deep flexion.
The patient can be positioned slightly more anterior on the operating table than with a standard posterior approach – this allows the operated leg to be adducted over the edge of the table if needed.
The foot is raised during the operation either on a dressed mayo table (my preference as it can be adjusted for height) or a foam bolster.
Standard basic hip instruments are used along with SuperPath® specific trays.













































Post operative rehabilitation is similar to traditional hip replacement techniques with some modification:
Minimal or no post operative restrictions are required regarding range of movement. Patients are told to do whatever feels comfortable but obviously extremes of range of movement should be ‘tested’ gently.
Recovery has been proven to be faster with regards time to coming off crutches, time to returning to driving and returning to work. (reference 3)
If anything, patients often have to be held back from too much activity as this will often cause some short term muscular and soft tissue problems such as Psoas tightness.

The results of this technique can be seen in several papers (shown below). These confirm the initial safety of the technique during the learning curve and the short term recovery benefits. Long term data is still required to confirm the longevity of implant survival and show any subtle improvements in long term function.
Reference 1 – Perioperative outcomes for nearly 500 consecutive Supercapsular percutaneously-assisted total hip replacements. Chow J, Fitch D e-poster, 28th ISTA, Vienna, October 2015
Reference 2 – Gofton W, Chow J, Olsen KD, Fitch DA. Thirty-day readmission rate and discharge status following hip arthroplasty using the supercapsular percutaneously-assisted total hip surgical technique. Int Orthop 2015;39:847-51.
This paper compares the results of almost 500 SuperPATH cases performed by 3 separate surgeons against the nationally published data for Canada and North America. The length of stay was reduced from 3.3 days (American) and 5.0 days (Canada) to 1.6 days. The 30 day readmission rate was reduced from 4.2% to 2.3%. Although this has economic implications in the American system (due to bundled payments) it is also a sign of surgical safety and low early complication rates. The discharge status was significantly improved with 95.3% of patients being discharged home rather than to nursing facilities (usual in over 30% of American patients). Complication rates were shown to be low confirming the safety of the technique.
Reference 3 – Qurashi S, Chinnappa J, Rositano P Asha S. SuperPATH Minimally invasive total hip arthroplasty – An Australian experience. JISRF, Reconstructive review. 2016;6:2
This retrospective review of the first 100 cases at 1 year follow up concentrated on return of early function. Within 2 weeks 86% of patients were walking without aids and 84% were able to dress independently. 81% of patients were driving within 4 weeks and 52% of those who worked pre-op returned to work within 2 weeks
Reference 4 – Percutaneously assisted total hip (PATH) and Supercapsular percutaneously assisted total hip (SuperPath®) arthroplasty: learning curves and early outcomes. Rasuli KJ, Gofton W; Ann Transl Med. 2015 Aug;3(13):179
Reference 5 – Della Torre PK, Fitch DA, Chow JC. Supercapsular percutaneously-assisted total hip arthroplasty: radiographic outcomes and surgical technique. Annals of Translational Medicine. 2015;3(13):180.
This publication describes the surgical technique in detail and the early results from the design surgeon. The post operative radiographs from the surgeons learning curve were examined and show good accuracy of implant positioning. This is important as previous ‘minimally invasive techniques’ have been criticised for poor long term results due to poor implant positioning.
Reference 6 – Gofton W, Fitch D. In-hospital cost comparison between the standard lateral and supracapsular percutaneously-assisted total hip surgical techniques for total hip replacement. Int Orthop. 2015;40:481-85.
This paper compares the cost of care between a group of 49 SuperPATH patients and a group of 50 Lateral approach patients from the same institution. The mean length of stay was 2.1 days in the SuperPATH group compared to to 5.1 days in the lateral group.
This paper compares the results of almost 500 SuperPATH cases performed by 3 separate surgeons against the nationally published data for Canada and North America. The length of stay was reduced from 3.3 days (American) and 5.0 days (Canada) to 1.6 days. The 30 day readmission rate was reduced from 4.2% to 2.3%. Although this has economic implications in the American system (due to bundled payments) it is also a sign of surgical safety and low early complication rates. The discharge status was significantly improved with 95.3% of patients being discharged home rather than to nursing facilities (usual in over 30% of American patients). Complication rates were shown to be low confirming the safety of the technique.
Reference 3 – Qurashi S, Chinnappa J, Rositano P Asha S. SuperPATH Minimally invasive total hip arthroplasty – An Australian experience. JISRF, Reconstructive review. 2016;6:2
This retrospective review of the first 100 cases at 1 year follow up concentrated on return of early function. Within 2 weeks 86% of patients were walking without aids and 84% were able to dress independently. 81% of patients were driving within 4 weeks and 52% of those who worked pre-op returned to work within 2 weeks
Reference 4 – Percutaneously assisted total hip (PATH) and Supercapsular percutaneously assisted total hip (SuperPath®) arthroplasty: learning curves and early outcomes. Rasuli KJ, Gofton W; Ann Transl Med. 2015 Aug;3(13):179
Reference
- orthoracle.com



