
Learn the MCP joint fusion of thumb (tension band wiring technique) surgical technique with step by step instructions on OrthOracle. Our e-learning platform contains high resolution images and a certified CME of the MCP joint fusion of thumb (tension band wiring technique) surgical procedure.
The thumb consists of three joints; the carpometacarpal joint(basal joint), metacarpophalangeal joint and the interphalangeal joint. Whilst the basal joint is a saddle joint which allows movements in multiple planes, the other two are hinge joints which allow flexion and extension. The metacarpophalangeal (MCP) joint provides stability for pinch grip. The range of movements of this joint do vary between individuals and in some people the joint has very limited natural flexion.
This joint can be effected be trauma and degenerative conditions. One common traumatic pathology which can lead to degenerative joint change here is injury to the ulnar collateral ligament which in the acute setting is called ‘Skier’s thumb’. If diagnosed in time this ligament can be repaired. Chronic laxity of the ligament due to repeated stressing is known by the eponym ‘Game-keeper’s thumb.’
The common degenerative pathologies effecting the MCP joint are osteoarthritis and rheumatoid arthritis. In osteoarthritis the joint develops inflammation and stiffness and commonly remains fairly well aligned. In contradistinction with rheumatoid arthritis complex deformity ranging from a Boutonniere to a Swan neck deformity can be associated with the degenerate joint.
The most definitive end stage surgical treatment for pathological conditions that result in severe MCP joint degenerative change (with or without deformity) is fusion. High levels of function can be expected as long as the remaining joints are functioning well. Replacements, though a technical possibility, have a tendency to early failure and sub-optimal function due to the high functional requirements of the thumb MCP joint.
There are several common methods for fixing an MCP joint fusion including K-wires, tension band-wiring, screw fixation alone and plate and screw fixation. Each of the techniques have their advantages and disadvantages.
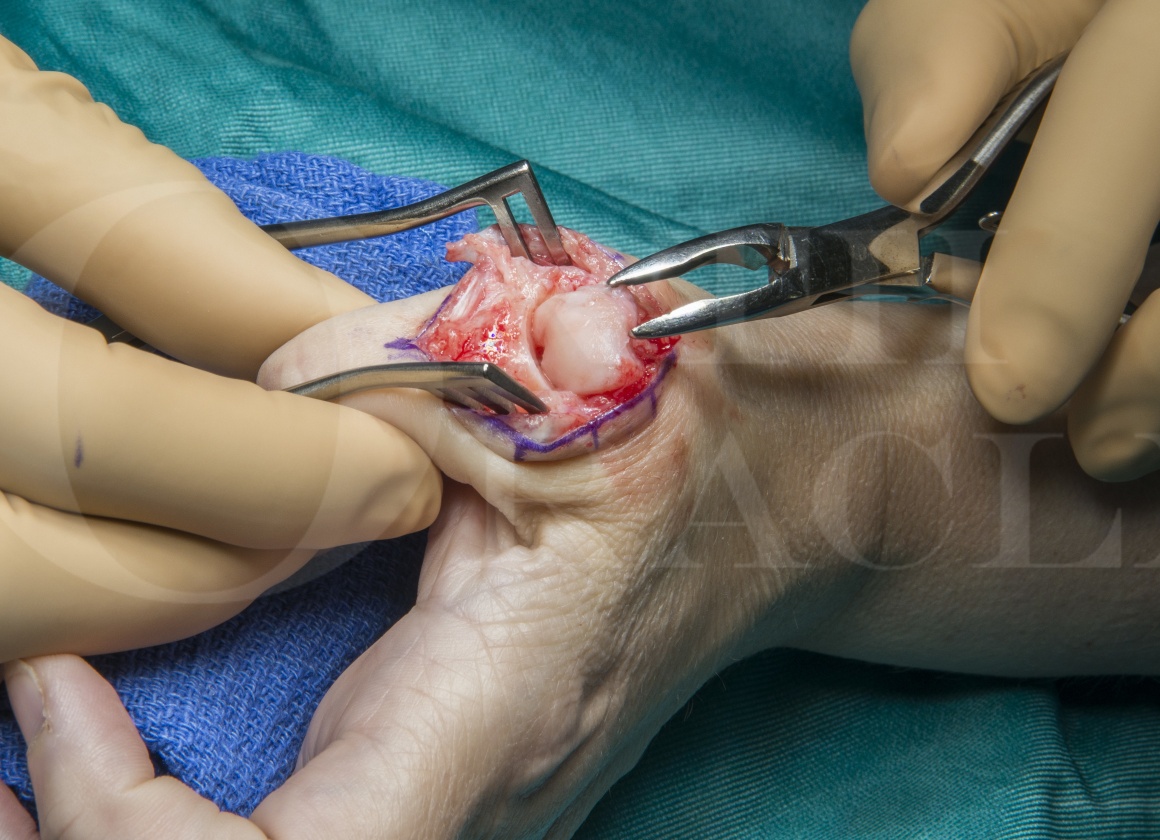
The case below illustrates the use of tension band wiring for performing a fusion of the MCP joint in a patient who has osteoarthritis and ulnar collateral laxity of the joint.

INDICATIONS
The common indications for fusion of the MCP joint of the thumb are:
Osteoarthritis
Rheumatoid arthritis
Other inflammatory arthritis such as Psoriatic arthritis
Chronic ulnar collateral laxity
Traumatic injury to the joint where the joint surface cannot be reconstructed
SYMPTOMS & EXAMINATION
A detailed history regarding the patient’s symptoms has to be elicited. The type and severity of pain and the functional limitations should be noted. History of previous treatment such as splints and intra-articular steroid injections should be asked. If these options have not been tried they can be offered to the patient.
Examination includes the upper limb in general looking at movements of shoulder, elbow and wrist and specifically at the thumb MCP joint. Swelling and tenderness around the joint is noted. Laxity of the ulnar collateral ligament is checked. Movements of the CMC joint and IP joints are checked. The usual symptoms are pain and stiffness of the joint. The is worse on pinching using the thumb or making a making a fist indication that the pain is on loading the joint.
IMAGING
Investigation is mainly through imaging. Plain X-Rays are usually sufficient to diagnose arthritic changes. In early cases ultrasound scan and MRI can help to identify subtle changes.
ALTERNATIVE OPERATIVE TREATMENT
For fingers, MCP joint replacement remains an option using either Silicone implants or the Pyrocarbon implants. However for the thumb, joint replacements do not work well as the forces going through the joints are too much and the joints wear out quickly.
Though Tension band wiring is chosen in this case there are alternative methods for fusing the MCP joint. These include plates and screws, headless compression screws, K-wires alone, staples and lag screws. My reasons for using Tension band wiring are that it has high union rates and that the metal work is not prominent as in plates.
NON-OPERATIVE MANAGEMENT
Splints and intra-articular steroid injections help in symptomatic management.
CONTRAINDICATIONS
The only absolute contraindication is an infection in the vicinity of the operation. Relative contraindications include co-morbidities which make anaesthesia risky.

The procedure can be carried out under Regional anaesthesia or General anaesthesia. The arm is positioned over a hand table with an upper arm tourniquet in place. A single dose of intravenous antibiotic is administered. Flucloxacillin 1gm is the antibiotic of choice and in patients allergic to Penicillin, Clindamycin 500mg in given.







































Patient is discharged home the same day with advise to elevate the arm in a sling for 24 hours. Patient is reviewed in the clinic in one week when the dressings are changed. A POP cast is used for 4 weeks extending from mid forearm to the middle of the proximal phalanx of the thumb, allowing interphalangeal joint movements.
At 5 weeks, POP cast is removed and check X-Rays are taken to look for union. If there is no solid union, a hand based thermoplastic splint is provided for further support for another 4 weeks and check X-Rays taken again.
Patients can get back to normal activities including driving at 6 weeks.
If there is limited flexion of the interphalangeal joint, hand physiotherapy is started through active and passive mobilisation. If at the end of 6 weeks of hand therapy, there is no improvement, removal of the metal work used for fusion and an extensor tenolysis is performed.

Lutsky KF1, Edelman D1, Lebowitz C2, Matzon JL1, Beredjiklian PK1. Union Rates and Complications After Thumb Metacarpophalangeal Fusion. Hand (N Y). 2018 Jul 1:1558944718784025. doi: 10.1177/1558944718784025.
There were 56 thumbs in 53 patients (42 women and 11 men) including 12 TBW and 44 PS. The mean age was 60.9 years, and follow-up was 32.4 months. Twenty-eight of 44 plates were nonlocking, and 16 were locking. Of the locking plates, 7 of 26 used all locking screws, and 9 of 26 had a combination of locked and nonlocked screws. The mean flexion angle for TBW was 16.5° and PS was 12.8°. The mean coronal angle for TBW patients was 4.0° ulnar and PS was 2.5° ulnar. The overall union rate was 95%. There were 12 complications, 9 in the PS group. The TBW complications were painful hardware requiring removal. Eight complications in the PS group occurred in patients with locked plates. Five of the delayed or nonunions occurred in patients with locked plates and 4 of these were in plates with all screws locked.
Complications using PS or TBW are not infrequent. Alignment with both techniques is similar, but use of locked plates specifically increases the rate of delayed or nonunions. We do not recommend routine use of locked plates for fusion of the thumb MPJ.
Hagan HJ1, Hastings H 2nd. Fusion of the thumb metacarpophalangeal joint to treat posttraumatic arthritis. J Hand Surg Am. 1988 Sep;13(5):750-3.
Thumb metacarpophalangeal (MCP) fusion to treat posttraumatic arthritis is retrospectively reviewed in 18 patients, 16 of whom were examined and functionally tested, with an average follow-up of 18 months. All patients were satisfied. There was 100% fusion in an average of 59.9 days. Preoperative disabling MCP pain was present in all patients, and mild postoperative pain and difficulty in picking up small objects were present in 78%. Results did not depend on position of fusion or preoperative arc of MCP motion. Key pinch strength was significantly increased by fusion. Complications included four pin tract infections without sequelae and three cases of prominent tension band hardware, which were removed in two.
Stanley JK1, Smith EJ, Muirhead AG. Arthrodesis of the metacarpo-phalangeal joint of the thumb: a review of 42 cases. J Hand Surg Br. 1989 Aug;14(3):291-3.
42 arthrodeses of the metacarpo-phalangeal joint of the thumb in 34 patients have been reviewed at a mean of 22.5 months after operation. Where bone stock allowed, Omer’s chevron arthrodesis was used. 83% of these operations were judged to have been successful by our patients, most of whom were suffering from inflammatory joint disease. Some patients had very poor pinch pressures when reviewed, but only those with persistent instability or pain were disappointed. All arthrodeses were fixed in flexion; although the angle varied, no ideal position was identified.



