
Dupuytren’s contracture is a relatively common condition which causes a histological alteration in a number of fascial structures within the palmar surface of the hand.
It is a clinical diagnosis and only rarely when there is a single nodule which has not caused any contracture in the early stages can it be difficult to diagnose.
75% of cases occur in the ulna 2 digits.
There is no current cure for the disease however there are 4 main groups of treatment options to improve contractures. These options are needle fasciotomy, fasciectomy, dermo-fasciectomy and collagenase injections. Within the fasciectomy group terminology becomes confusing with many terms being used synonymously despite original descriptions differing. Examples are focal, segmental and limited fasciectomy. There is also variation in a dermo-fasciectomy with a small fire-break skin grafts or a larger graft covering a clear anatomical section e.g. volar finger between MCPJ and PIPJ creases.
In addition, adjuncts to surgery such as temporary external fixators or salvage options such as amputation or joint arthrodesis are also included in the Dupuytren’s treatment armamentarium.
Fasciectomy, to be shown in this case can be performed under local, regional or general anaesthetic dependant on the disease pattern and anaesthetic support. The procedure is performed under tourniquet control and a patient normally is treated in plaster cast until their 1 week review where they start mobilisation and 3 months night splinting with the hand therapists.
Complications include failure of complete correction (common with severe PIPJ disease where the joint capsule and ligaments are contracted), recurrence (very common eventually with rates of 10-50% at 5 years depending on disease severity, joint involved and treatment method used), neurovascular injury (rare however increasing common the greater the number of revision surgeries at a single site), infection and stiffness. Graft failure in dermo-fasciectomy and allergy to collagenase are additional complications that are an additional risk with other methods mentioned.

Pathology and Anatomy
Dupuytren’s disease is an inherited autosomal dominant trait with variable penetrance and expressivity. Normal fascia is composed mainly of type I collagen. In Dupuytren’s there is a increase of type III collagen (as also seen in wound healing) and myofibroblasts which are a contractile cell derivative from the fibroblast.
With this contractile potential the normal anatomical ‘Bands’ within the hand can become contracted ‘Cords’.
In addition to ‘Cords’, ‘Nodules’ are seen when a bulk of Dupuytren’s tissue appears in one site and ‘Pits’ are seen when the skin fibres contract and pull small areas of skin down towards the deeper cords in the palm.
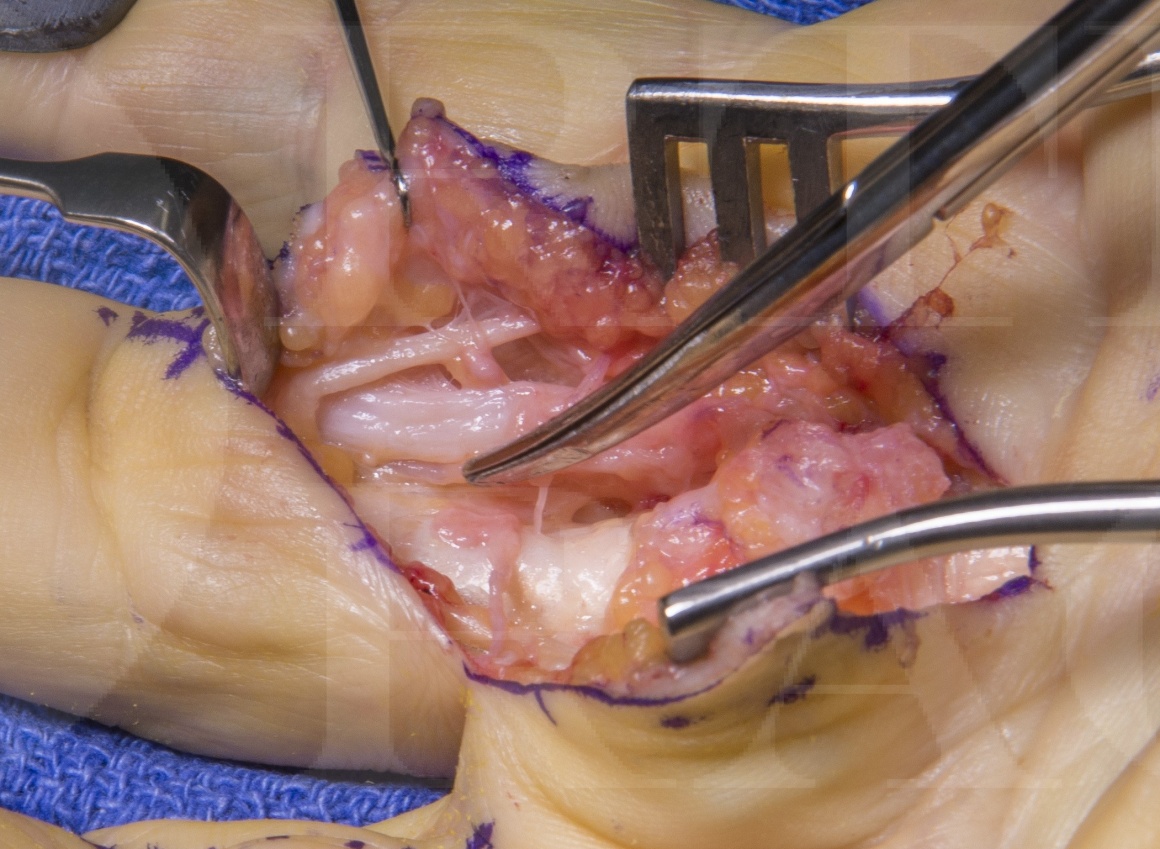
Examples of the anatomy will be shown in the surgical pictures however as an overview the bands/cords are:
Pretendinous (band/cord) – a continuation of the palmaris longus and palmar fascia which is in line with each digit and inserts around the flexor sheath at the level of the MCPJ crease (a central cord can continue in this line along the flexor sheath to the DIPJ).
Natatory (ligament/cord) – transverse cords which span between the web spaces blending with the pretendinous band/cord and spiral band/cord
Spiral (band/cord) – longitudinal structure superficial to neurovascular bundle (NVB) crossing from pretendinous band/cord to blend with lateral digital fascia, when contracted this pulls the lateral digital fascia/cord centrally and as the NVB is enclosed by Grayson’s and Cleland’s ligaments which are attached to the lateral digital fascia the NVB is then pully more centrally in the finger at the level of the MCPJ crease.
Lateral digital (fascia/cord) – longitudinal structure close to the skin running almost up the lateral midlines of the fingers attached to Grayson’s and Cleland’s ligaments.
Retrodigital (fascia/cord) – distal continuation of lateral digital fascia/cord which may cause DIPJ contracture.
Commisural (band/cord) – similar to Natatory but of the 1st web space
Legueu and Juvara (septa/cord) – vertical structures which separate the distal palm into sections with NVB and lumbrical then flexor sheaths in alternating sections.
Grapow (fibre/cords) – small vertical structures which tether the palmar skin to the deeper fascia and provide stability of the skin and cause pitting when contracted.
INDICATIONS
Dupuytren’s contracture effects around 2 million people in the UK.
A patient will present for treatment usually for 3 reasons.
They have lumps in the palm and are unsure of the diagnosis and may be worried about a diagnosis or cancer. – These patients can be reassured based on a clinical diagnosis, educated on the condition and discharged.
They are aware of the diagnosis and the tightness of the palm or nodules are a nuisance but no clear fixed flexion deformity – these patients are best educated about the condition and the likely recurrence rates and therefore avoidance of very early surgery to avoid scarring and increased future complications of repeat surgery. If they still would like intervention in specific cases (e.g. professional pianist who’s span is reduced or tree surgeon with large nodules but no contracture making gripping difficult and climbing unsafe – reasonable surgical indications) they have two options in the UK. One is to have treatment in the private sector and the other is for the surgeon to apply for specific funding on individual grounds for the treatment to the funding body.
The patient has a contracture of the digit causing dysfunction. In the UK patients can undergo funded treatment for Dupuytren’s contractures based of certain guidelines (often falling under ‘Procedures of limited clinical value’). In the authors region this states if there is a progressive PIPJ contracture or an MCPJ contracture of 30 degrees or more then treatment can proceed. These value are often the point at which dysfunction is increasing due to the contracture.
Symptoms
Dupuytren’s disease is a non-painful condition. Although the condition can be itchy or sore when active proliferation is taking place, or painful when gripping if a large nodules are compressed, if pain is a main feature of the presentation then a rare but serious diagnosis of fibrosarcoma should be excluded.
Dupuytren’s contracture is a spectrum of severity and can range from a mild inconvenience to a disabling condition with all ten digits severely affected.
Patients complains of aching or cramping in the hands, a feeling of tightness and the inconvenience of the contracted digit of poking then in the eye when washing their face, catching on their clothes when trying to get money out of their pocket and sticking on door handle after they have opened them.
The Dupuytren’s diathisis is a collection of signs and conditions which are seen to suggest a worse prognosis in terms of disease progression and recurrence. This is made up of age <50, male, bilateral disease, radial sided disease (thumb/index finger), family history and ectopic disease. Ectopic sites include the dorsal PIPJ nodules (Garrod’s pads), penile fibrosis (Peyronie’s disease), plantar fibrosis (Lederhose’s disease).
Examination
Inspection usually reveals cords, nodules and pits within the palms and fingers.
It should be noted from the history which specific fingers are troubling the patient especially in more severe disease when all fingers are affected and multiple treatments and recurrences have already occurred.
Joint contracture angles should be measured and recorded and it is useful to isolate each joint and record the combined and individual joint contractures. This is performed with a small finger goniometer on the dorsum of the finger. Initially the whole finger is extended maximally and the joint angles recorded. Following this the MCPJ is fully flexed and PIPJ maximal extension is recorded then the PIPJ is maximally flexed and the MCPJ extension angle recorded.
This differential will help the surgeon identify if there is a spanning cord contracting both joints and help with prognosis to predict the post-operative correction.
As a general rule all MCPJ contractures caused by Dupuytren’s no matter how severe will be corrected by treatment. Any PIPJ contracture above 60 degrees is likely to remain with some contracture post treatment. This is due to the collateral ligament and volar plate contractures which can be released intra-operatively to provide a greater extension but at greater risk of joint stiffness, and loss of flexion.
After previous surgery a digital Allen’s test (as for Allen’s test at the wrist the finger can be squeezed by the examinar to exsanguinate and both digital arteries pressed upon and released one at a time first starting with Radial then on the second time starting with the Ulnar.. The rate of reperfusion should be noted and if a significant difference noted between sides then a possibility of previous arterial injury should be considered) and assessment of sensation are also useful to record if further intervention is being planned.
Further examination of ectopic sites can be undertaken if necessary although usually only the dorsal PIPJ disease of Garrod’s pads is reviewed.
Investigations
There are no formal investigations for Dupuytren’s disease unless there is a concern regarding pain and a possible diagnosis of sarcoma. In this case a USS or MRI may be performed. This may also be necessary in an isolated nodule where diagnosis is unclear.
Non-operative Management
The best non-operative treatment is patient education and reassurance which includes advice on the stage of disease progression which treatment is advised.
Non-operative management with splinting or physiotherapy have not shown to be affective. Radiotherapy is one option used to prevent disease progression however the evidence on its effectiveness is limited. The author does not use this in their treatment pathway.
Alternative operative Management
As discussed the alternative treatment options to fasciectomy include – needle fasciotomy (aponeurosis), collagenase injection, dermo-fasciectomy, amputation and an adjunct of temporary external fixation or joint arthodesis.
Contraindications
A relative contraindication to fasciectomy is multiple previous surgeries with rapid recurrence when alternative treatment options such as joint arthrodesis or amputation may be a better consideration.

Pre-operative preparations and Equipment
The operation can be performed under local, regional or general anaesthetic.
No antibiotics are used and thromboprophylaxis is not required unless the patient is under a GA for a >90mins.
A pre-opertive checklist is completed and the patient is supine with the arm placed on an arm board. An upper arm tourniquet is used and set to 250mmHg (if local anaesthetic and adrenaline are used for anaesthesia the tourniquet may not be necessary).
The hand is held in a lead hand or equivalent and the skin incisions marked.
Plaster cast is used post-operatively.




























Following the procedure the patient is provided with a Bradford sling to elevate the hand and is reviewed in the dressing clinic within a week.
At the clinic the plaster cast is removed, dressing changed and wound reviewed for any signs of infection.
In the cases of dermo-fasciectomy the skin graft dressing is not review until 10-14 days however splinting will still take place with mobilisation delayed until the graft check.
The hand therapy team with then fashion a thermoplastic night splint to maintain extension and start mobilisation exercises.
The patients will be seen weekly by the hand therapist until full flexion achieved.
The patient is reviewed in the consultant clinic at 3 months and if all is well discharged at this point.

As noted all MCPJ contractures are expected to regain full range of movement. The more severe the PIPJ contracture the less likely a full correction will be achieved. In addition the prolonged flexion of the PIPJ appears to attenuate the central slip slightly and despite a very good correction there may be a lag due to the extensor function which it is hoped will resolve with night splinting.
Complications
Surgical Complications Associated With Fasciectomy for Dupuytren’s Disease: A 20-Year Review of the English Literature K. Denkler. Eplasty. 2010; 10: e15.
This study found 28 papers which included complication data revealing a overall range from 3.6% to 39.1%. Major complications in 15.7%, including digital nerve injury 3.4%, digital artery injury 2%, infection 2.4%, hematoma 2.1%, and complex regional pain syndrome 5.5%. The also saw a trend to a 10 fold increase in digital nerve injuries when comparing primary to revision surgery.
Five-year results of a randomized clinical trial on treatment in Dupuytren’s disease: percutaneous needle fasciotomy versus limited fasciectomy. van Rijssen AL1, ter Linden H, Werker PM. Plast Reconstr Surg. 2012 Feb;129(2):469-77.
This RCT with 115 hands treated revealed a recurrence rate for needle fasciotomy (84.9 percent) was significantly higher than in the limited fasciectomy (20.9 percent) (p < 0.001).



